AMWA is a leading advocate for gender equity, women’s health, and research.

Promote Gender Equity
We advance gender equity through advocacy that ensures fairness in opportunity, pay, and workplace culture.

Advance Women’s Leadership in Medicine
We address the gender gap in leadership to promote equitable representation in healthcare.

Address Healthcare Disparities
We advocate for policies that reduce healthcare disparities and promote equitable access to healthcare.
The American Medical Women’s Association (AMWA) addresses issues impacting women in medicine — from gender equity and infertility to sexual harassment and physician suicide — bringing them to the forefront of the national agenda. As women physicians and advocates for the health of women, we are uniquetly positioned to change the culture of medicine within the communities in which we serve.
Our advocacy efforts are also driven by the needs of our members, so find an area of interest and put your passion to action.
Events
(Videos available in the AMWA Member Learning Hub)
Civic Engagement in Health Care Settings | Oct. 20, 2022
in partnership with Civic Health Alliance
Civic engagement through voting is vital to the health of our communities. It allows us to influence policy about resourcing and regulation of our healthcare system, including provisions that impact social determinants of health. Physicians have historically not been active voters, participating at a rate lower than that of the general population — it’s time to change that! ALSO – physicians and other healthcare providers interact with many, diverse members of their communities and thus are uniquely positioned to impact civic engagement.
Panelists:
Dr. Theresa Rohr-Krichgraber
(President, American Medical Women’s Association,
Jeanne Ayers, R.N., M.P.H.
(Executive Director, Healthy Democracy, Healthy People),
Jessica Rebeza, MS, CHES
(M3, St George’s School of Medicine)
Event Moderator:
Russia Chavis Cardenas, MPP
(Director of Strategy and Partnerships, Civic Health Alliance)
AMWA Areas of Advocacy

Civic Engagement
Physicians have voted less than most Americans. Let’s change that by leading voter engagement and healthcare advocacy.

Legislative Advocacy
Stay informed. Use your white coat to influence health policy—take action through our 2 minute Advocacy Action Hub.

Equity
Learn about our Gender Equity Task Force (GETF) and Justice, Equity, Diversity, and Inclusion (JEDI) Council .

Women’s Health
For over a century, AMWA has advanced women’s health, focusing on education, prevention, and access
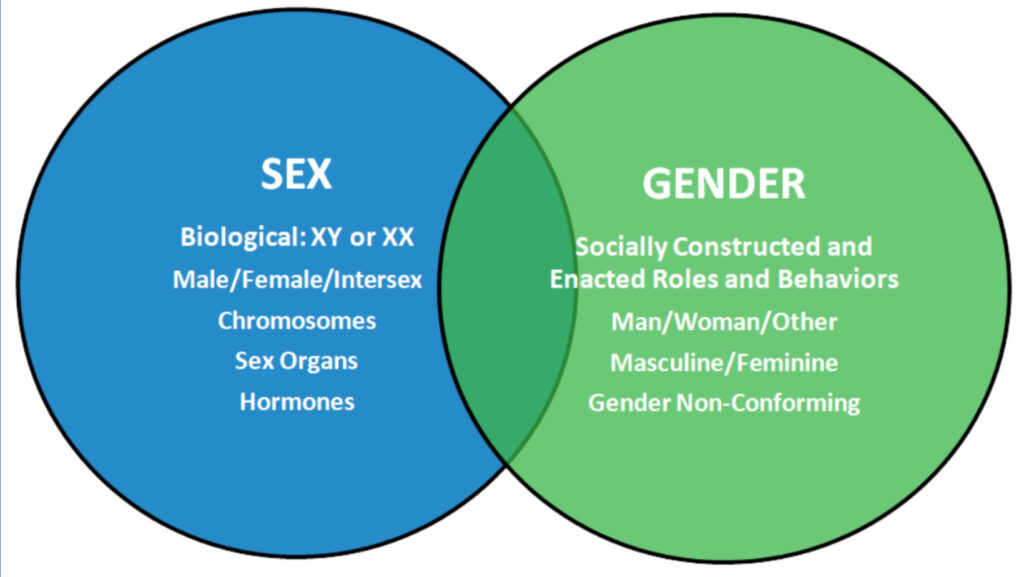
Sex & Gender Specific Health
AMWA’s Sex & Gender Health Collaborative and Education Summits promote awareness of sex differences in clinical care.

Reproductive Health
AMWA and the Reproductive Health Coalition are working to ensure reproductive care access without legislative interference.