Health Equality vs. Health Equity
written by: Sai Kurapati
Up until freshman year of college, I considered myself an avid advocate for health equality. Only after coming to Brown and gaining opportunities to immerse myself in real-world activities of advocacy, did I realize what I was actually passionate about was promoting health equity. Often mistakenly used interchangeably, equality and equity, though inextricably related, are quite distinct. The Equality and Human Rights Commission defines equality as the distribution of the same resources and opportunities to every individual across a population. Equity, on the contrary, is defined by the World Health Organization as the customized distribution of resources and opportunities across a population to ensure no subset of groups are at a particular disadvantage over others in achieving their maximum potential.
In other words, while equity accounts for disparities, equality does not. When it comes to healthcare, this difference becomes especially magnified and thus, even more important to address in discussion surrounding advocacy for equal access and outcomes. Health initiatives that solely focus on distributing equal resources are not sufficient, as the burden of disease does not simply afflict every individual in society in the same manner. For that reason, biomedical and social influences on healthcare access and outcomes must be addressed and resources distributed accordingly. The biomedical model of disease attempts to discover ultimate causes of patient’s sickness, whereas the social model of disease emphasizes investigating proximate factors—aspects of a person’s lifestyle that may expose them to greater risks of contracting disease.
Taking the personalization of medicine and uniqueness of each patient story into consideration, the most impactful method of improving health outcomes in a community is through holistically tending to the individualized needs of the population. This entails introducing interventions that confront causes of health disparities— preventable differences in various aspects of health status in a population— and acknowledging the role of social determinants in shaping disease. Equitable distribution of opportunities and resources involves understanding how non-biomedical factors such as race, ethnicity, gender identity, geographic location, culture, and socioeconomic status contribute to disparities in disease incidence, prevalence, and mortality. Often gone overlooked in traditional medicine, such social epidemiological influences on disease have been significantly more integrated into modern medical practices. Raising the public’s awareness of the increasing role of non-physiological influences on disease is an important part of health equity advocacy, because it helps to break the stigmatized assumption of disease as only “physical”.
The diagram to the right is a powerful depiction of the difference between equality and equity obtained from Allies for Reaching Community Health Equity (ARCHE). Equal distribution of resources (the same number of crates in this scenario) to every individual in a community does not translate to the delivery of fair, nondiscriminatory aid. Only by adjusting for the individualized 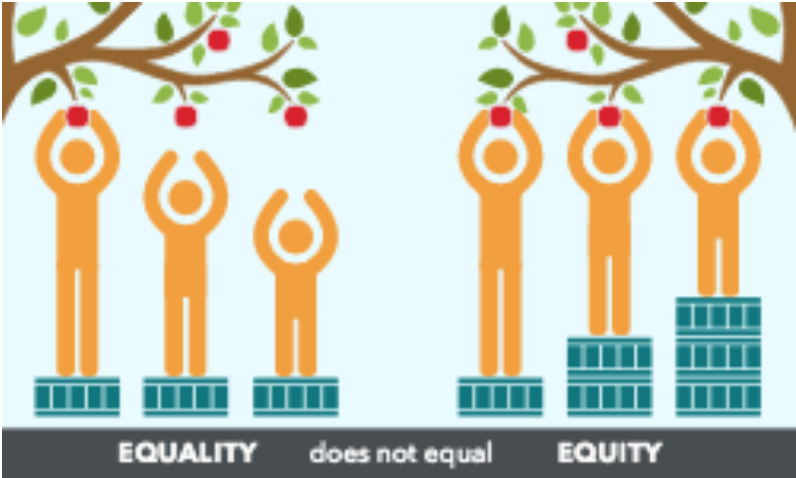 needs of a community and resourcing a different number of crates to each person based on their personal status can disparities in the access to resources (apples in this scenario) within a group be eliminated. Equality does not acknowledge the possibility for a community to be composed of a mixed population of more and less advantaged members. The shortest person in the illustration only has an equal opportunity of attaining an apple when resources are distributed equitably, not equally.
needs of a community and resourcing a different number of crates to each person based on their personal status can disparities in the access to resources (apples in this scenario) within a group be eliminated. Equality does not acknowledge the possibility for a community to be composed of a mixed population of more and less advantaged members. The shortest person in the illustration only has an equal opportunity of attaining an apple when resources are distributed equitably, not equally.
Likewise, disparities in quality of care and health outcomes can most effectively be mitigated through efforts promoting health equity rather than equality. The use of intersectional perspectives when attempting to make different aspects of medical care more equitable, reinforces the powerful role of social determinants in influencing human conditions of disease beyond traditional biomedicine. Disseminating appreciation for the distinction between equality and equity as it relates to medicine is the first step to achieving health equity, as knowledge is the basis for change. For such reasons, it is critical that advocates internalize what a truly unprejudiced healthcare system entails. Those like me who are passionate about promoting health equity must stay aware of their language as they engage in activities promising to further fair access to quality medical care and health outcomes. Understanding the relationship between equality and equity evinces the difference that two letters can make on delivering the rightful healthcare they deserve to thousands of lives.